Gastroesophageal reflux disease
What is gastroesophageal reflux disease or GORD?
Gastroesophageal reflux (GOR) is a common condition in infants and babies where the contents of the stomach moves up and into the feeding tube (oesophagus) and sometimes into the mouth. This is very common and is a normal process. If however the baby becomes symptomatic (eg experiencing pain or weight loss) then we call it Gastroesophageal reflux disease (GORD). Note that in America,because of the spelling of oesophagus, this becomes “GERD”.
This article was written by Dr Tim Ubhi, a Consultant Paediatrician with over 25 years experience in Paediatrics & Child Health. We hope that it gives you a better understanding of this topic and also how the symptoms may overlap with other conditions.

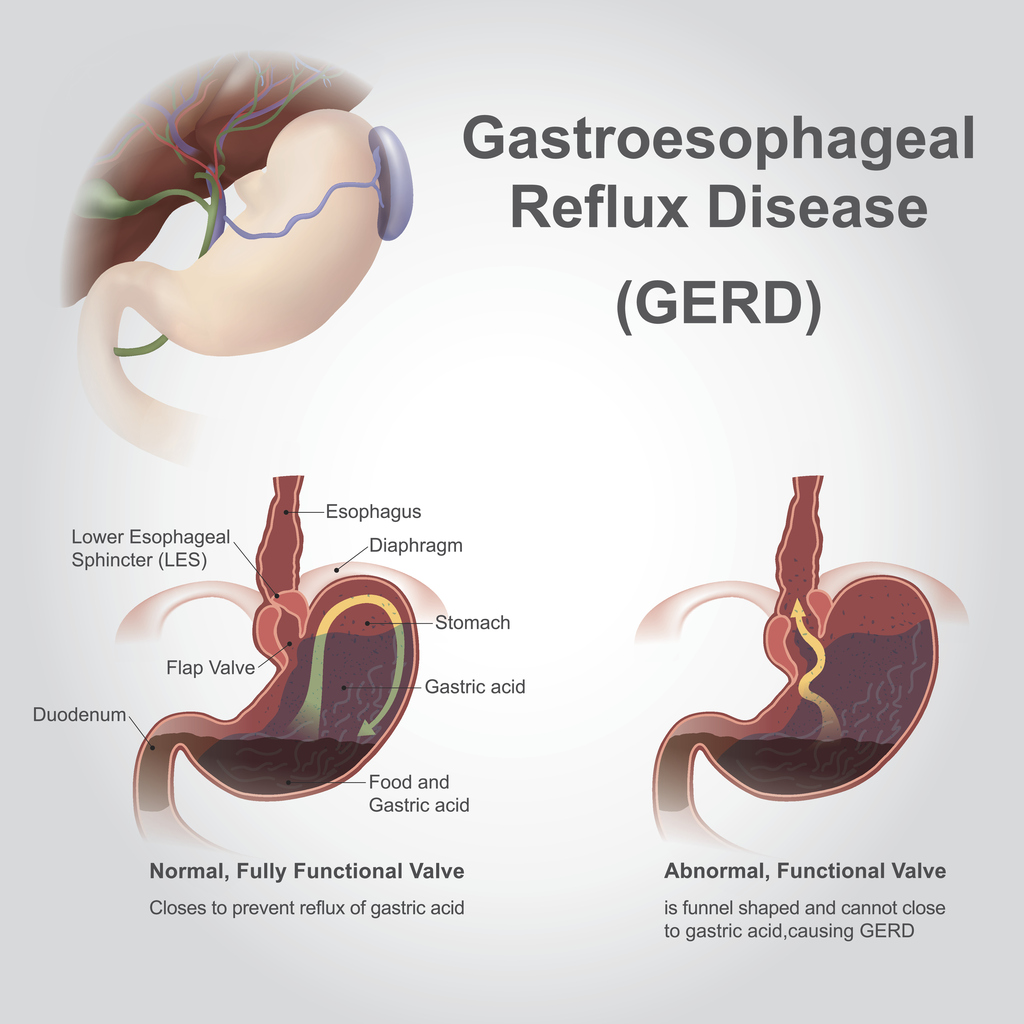
The picture above shows the normal position of the feeding tube (oesophagus) and the stomach. The picture below shows how the valve at the bottom of the feeding tube fails in gastroesophageal reflux disease.
Signs & symptoms
Regurgitation appears to be commonest around 4 months of age with 60% of children having symptoms. This decreases to about 20% by 7 months of age and then nearly all children are symptom free by 1 year of age.
Gastroesophageal reflux (GOR) is different to gastroesophageal reflux disease (GORD). GOR is very common in babies and peaks at around 4 months of age. Refluxing without symptoms is normal.This is sometimes called “regurgitation”. It only becomes a problem (and hence is termed GORD) when it begins to impact on the health of a baby. This may be with evidence of pain after feeding, weight loss or other features.Remember to look out for the warning signs or “red flags” which are listed below.
Regurgitation occurs in about 50% of 0-3 month olds and gradually decreases to about 5% at 12 months of age. So you can see that time is a great healer.
Gastroesophageal reflux disease usually improves with the addition of thickeners, the introduction of a cows milk & soya free diet, or with the addition of anti-acid therapy. Note that if you are allergic to cows milk protein you have a roughly 1 in 2 chance of also being allergic to soya protein.
Red flags
It is important to determine if there is an underlying problem that is causing the reflux.
Warning signs include
- Bile stained vomiting
- Vomiting blood
- Black tar like poo
- Onset of vomiting after 6 months
- Constipation or diarrhoea
- Abdominal pain
- Recurrent chest infection
- Large liver or spleen
- Neurological symptoms (eg muscle weakness)
- Rapidly increasing head circumference
- Fever or irritability
- Poor weight gain
Silent reflux
“Silent reflux” is a slightly confusing term which technically is described as “laryngeal-pharyngeal reflux”. This means that there is movement of stomach contents (that can be acidic) into the area around the throat and vocal cords. It is characterised by a hoarse voice, frequent throat clearing and coughing.
There is a suggested link between “silent reflux” and asthma as the movement of acid up the oesophagus can stimulate nerves that can then cause coughing and wheeze. Researchers are investigating the links between silent reflux and recurrent ear infections but this link has not as yet been proven.
Treatment
Treatment usually follows the following steps:
1.Ensure that there are no warning signs or red flags
2. If evidence of poor weight gain, distress with feeding, blood in stools or vomit, eczema or strong family history of allergic disease then consider a cow’s milk and soya free diet and review after 2-4 weeks to see if there has been any improvement.
3. If cow’s milk/soy allergy is not considered likely then add thickeners to formula milk or expressed breast milk.
Commonly used thickeners include “Carobel” and “Thick n’ easy”. (note that Gaviscon acts as a thickener in babies rather than as an anti-acid). Also stop any exposure to tobacco smoke because we know that tobacco smoke can worsen reflux.
4. If the addition of thickeners do not improve the symptoms then consider acid suppression using ranitidine or omeprazole for a 2 week period.
If this helps, then continue for 3 months. Because of the increased side effects with omeprazole we would recommend starting with ranitidine first.
5. If acid suppression treatment doesn’t work then blood tests should be carried out (including a screen for coeliac disease if exposure to wheat, rye or barley has occurred) and a referral for an endoscopy should be considered.
Occasionally patients will need evaluation in hospital but surgery is very rare in children under 1 year of age.
The following link will take you to the NICE guidelines for diagnosis and management of a child with gastroesophageal reflux disease:





